Do you have any clue what to do to treat yourself or others if someone is shot? Could you stop your own or someone else’s bleeding quickly enough to save a life? Are you familiar with the priority of treatment of various injuries? Those of us in the CCW/gun community place great value on self reliance. We believe that when seconds count, police are only minutes away. If you take that seriously, you should feel the same way about medical help. Most of us don’t treat this issue with the gravity it deserves. Beating the Reaper: Trauma Medicine for the CCW Operator by Dr. John Meade and “Sua Sponte” ($25 from One Source Tactical) is a great first step in educating yourself in lifesaving first aid. I bought the book last week and read it through in one sitting . . .
[FYI: graphic photos, all used with the authors’ permission, after the jump]
The authors of the book are both experienced in medical care in the context of a violent altercation. Dr. Meade is a board certified ER physician, EMS director, and instructor of Tactical Medics for SWAT teams. He also serves as a reserve officer on a SWAT team. Mr., well, “Sponte” is a Special Forces combat medic still active in the service and, as such, prefers a pseudonym. He has extensive experience treating injuries under fire in exotic locations around the world. While both authors are experienced treating injuries in the context of a fight, more importantly the authors have an ability to organize, present, and teach this material in a manner anyone can understand.

The book is short (131 pages of large font) and takes only two to three hours to read cover to cover. It clearly explains the evaluation and first treatment of a penetrating trauma in the context of an ongoing violent event. I come to the book as a surgeon with 10 years of training and 10 years of experience behind me. The information isn’t dumbed down, but the terminology is explained so that almost any lay person can understand it. I’ve always said that medicine is mostly common sense, and Beating the Reaper presents a very simple, common sense approach to initial treatment of injuries that anyone can learn and apply.
The chapter on tactics is probably the most unique part of a book. It’s certainly the first time I have ever seen the term “fire superiority” used in a first aid book. The point of the chapter: winning the fight is the best first aid, otherwise you and those injured around you are as good as dead.
Once you or any other “friendly” person is injured, your immediate action must be to increase the ferocity of the fight and focus on eliminating the threat, rather than on treating casualties or addressing your own wounds. If you don’t win the fight, you may all die.
The chapter gives some techniques for one-handed weapon manipulations for hand guns and rifles, self aid and buddy aid. The authors point out that ambulance crews are taught not to enter an unsecured area that could be dangerous to them. That means you and anyone with you may be on your own from an aid perspective until police secure the scene for the ambulance crew. That means the faster you can end the fight, the faster the professionals will be able to reach you with medical help. There’s also a brief discussion of cover vs. concealment, how and when to move an injured person and functioning in low light environments.

Chapter three gets the reader into heavy duty first aid, namely hemorrhage control and it’s worth the price of the book on its own. They go into some detail on the physiology of bleeding and follow up with several practical approaches to making it stop: direct pressure, pressure dressings, wound packing, hemostatic agents and tourniquets. The section on tourniquet use was extremely valuable, covering several different tourniquet systems including improvised tourniquets.
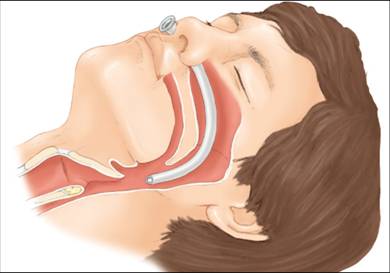
Chapters four and five cover airway management, breathing and chest injuries. Again, the physiology is discussed in plain layman’s terms followed by assessment and various simple maneuvers you can use to open and or maintain an airway, including how to use a simple device called a nasopharyngeal airway. Treatment of open pneumothorax and facial wounds is briefly discussed, too.
Next up is shock management and simple stabilization of orthopedic injuries, including improvised splinting.

The book ends with something we all should think about: how to put together a first responder trauma kit, as well as evaluating some of the commercial kits currently on the market. A medical/tactical glossary follows the final chapter.
It’s hard to quibble with the content. I would have loved to learn about other areas such as surgical airways, inhalation injuries, blast injuries, burn care, needle decompression of pneumothorax, etc. But those things distract from the main focus of this book which is how a lay person can perform simple, life saving initial injury care they’re likely to experience after a defensive gun use. I suspect volume two may get into a few of these areas.
Overall, this is a valuable resource for virtually anyone. The book is aimed squarely at the average Joe who may suddenly be put in a life threatening situation with nothing other than his wits and a few simple tools at his disposal. And while this kind of first aid is vital for just about anyone, it should be required reading for those carrying a firearm.



{kind=link}
This is important stuff. I’m a physician, albeit way out at the esoteric end of the science (radiology), but getting pimped for hours by surgeons during medical school about Advanced Trauma Life Support does tend to stick with you. I think I could keep someone alive long enough for better-trained folks to get there, knowing the anatomy helps some.
The real reason this is important is that people rarely fall over DRT from handgun wounds. Knowing how to control hemorrhage WILL mean the difference between surviving handgun wounds and not surviving them.
I have a commercial trauma first-aid pack that lives in my range bag. I figure that if accidents are going to happen, they’re going to be where the most rounds get fired on a regular basis. I look forward to reading this book, and will consider adding another trauma pack to the car…just in case.
Interesting.
There are a lot of first aid books out there, and I have above average medical training, but its good to see a review by some one in the medical field. From a lot of similar manuals I’ve got the distinct feeling that they’re either not telling me something, lying, or just incompetent…
Heckler & Koch used to run a CME course that covered treating wounded under fire. How to intubate with you & the wounded both lying prone, etc. My favorite thing about this CME course was that it said that if you didn’t have your own SMG, you could use one of HK’s. Not many CME courses ask you to bring 1500 rounds of 9mm.
Sadly, HK decided not to sponsor that one any more.
It’s a good book. I’m told the next book will go into somewhat more advanced stuff, like chest decompression. I took a class taught by both of the authors a few months ago, very good. The TCCC class I took somewhere else covered the more advanced stuff, but it was not nearly as well structured and had a lot more unproductive time or scenarios that were kind of dumb.
I keep a quick clot field trauma pack in my range bag and one in my car.
Also pays to be aware of legality issues if rendering first aid to another. In Pennsylvania, for example, Good Samaratin laws don’t kick in unless you’re a licensed professional OR you are first aid certified by Red Cross.
TTAG commentator Greg in Allston and I recently took a course in emergency trauma care for CCW holders. It was illuminating, and I hope to take another, more extensive course this year.
I hope that I will never need to use the training, just as I hope that I will never need to use a gun in self-defense. Still, it makes sense to me that I should plan for the worst while I hope for the best.
If I may put in a plug – there are trainings, geared toward those who go into the backcountry or work in rural settings, that are very good.
I think most folks are familiar with American Red Cross First Aid and CPR classes. But there is also the Wilderness and Remote First Aid class. Or you can invest your time and go for the ARC First Responder course. See http://www.redcross.org and/or contact your local ARC office
(For those working with youth groups in the Greater Houston Area, see http://www.scoutcpr.org for classes.)
Wilderness Medical Institute (WMI), part of the National Outdoor Leadership Schools (NOLS) has an excellent set of courses for various levels of first aid training. http://www.nols.edu/wmi/ has more information.
There may be more out there, but these are, to my knowledge, the best sources available to the civilian. Reading the book is fine. Taking a training class where you get your hands “bloody” is better.
The good Doc offers training in just that including live shooting and FOF scenarios I believe
http://www.suarezinternationalstore.com/traumamedicine.aspx
I’ll give up completely the sarc on this topic. If there is a gun in my car or in my hand late at night, my vest is there, and in the back uni-pocket are common forms of metal-ladder splint, tourniquet, valved chest patch, ‘israeli bandages’, celox, and a few other items. My son thinks it’s dubious. Such is inexperience. I’m 60, but my greatest traumas in life were watching untreated gunshot wound victims (2) 90 or so feet below me on a rope bleed out (extraction ropes, “strings”) before we could set down in a safer spot. We always carried chase medics along, and one of them, Yevich, then 20, edited a nice manual later in life, SOF Medical Handbook. What I learned then, amongst other things, was that many people ‘win gunfights’ but don’t live to tell about it. It happens in suburban houses, too. Knowing how to stop a hemorrhage, patch a sucking chest wound, or stabilize a compound fracture is worth the trouble. The book reviewed is a start. Any suggestions, Darren? Gunsite ought to include this kind of material. So many people can shoot so well, but haven’t got a clue what to do before the EMT gets there, when shot on the way to ‘winning.’ Enough. Good topic.
Like I said, yo soy radiologist. Give me a $1 million CT scanner and three-phase power and I can tell you everything that’s wrong with somebody, but I’m a lousy IV stick. I can hit arteries, those are simple, they pulsate, but other than doing an arteriogram that’s a skill that isn’t part of the standard trauma care package. About all you can do with an arterial stick is to get a blood gas, and without a lab that doesn’t tell you much you didn’t already know. I do not want anyone to get the impression that I am a field operator, I’m not only NOT primary care OR secondary care (surgeon), I’m tertiary care. I haven’t even intubated a live person, and hope never to have to. I think I could bluff my way through a cricothyoidotomy in an extreme emergency, but more from reading lots of thyroid ultrasounds, knowing the anatomy and having watched a M*A*S*H rerun.
That being the case, the standard trauma ABCs apply: Airway, Breathing, Circulation. Make sure the patient can breathe. If they can’t breathe, they’ll suffocate before they bleed out.
In terms of penetrating injuries to the extremities, the tourniquet is your friend. The thought used to be that tourniquets were only good for thirty minutes or so and that you risked limb loss, combat expereince in Iraq has shown that tourniquets are good for a couple of hours. The ABCs for penetrating injuries to the limbs really come down to Attain Bleeding Control. Tourniquets should be wider than you think, commercial & military tourniquets are 2″ wide. Get it above the GSW and tighten until the bleeding stops. The best thing to stop bleeding that isn’t arterial is pressure, clotting agents help but direct pressure will stop any bleeding that isn’t clearly arterial, and if pressure doesn’t work it’s tourniquet time.
As far as chest and abdominal wounds go, the problem with abdominal wounds is too much space and the problem with chest wounds can be not enough if you run into a “sucking” chest wound. The wound can act like a ball valve, inspiration pulls air into the space around the lungs and expiration closes the wound, trapping more and more air in the chest cavity until breathing stops or circulation is impaired. The solution is to actually open the wound a little more in that case so the ball-valving doesn’t continue, then cover the wound with an air-proof dressing. In the hospital that happens with a chest tube, improvisations can include using a needle higher up in the chest (air rises) to reduce pressure and bleed out the air in that cavity.
The problem with both the peritoneal cavity and the chest cavity is that most people only have 10 units (3.5L, more or less) of blood, and when you get down to 4-5 units you’re going to run into real problems. It’s relatively easy to lose that much into the peritoneal cavity or chest cavity from a penetrating injury in those places that goes unaddressed.
We biopsy the liver frequently with 18 ga needles, but in people with hepatic disease (cirrhosis, metastatic disease) even that can be fatal. And since the liver is relatively stiff it tends to crack & bleed like crazy when shot. Pressure is about all you’ve got in the field, so basically, don’t get shot in the liver.
The main reason to get ahead of bleeding, besides preventing circulatory collapse, is to avoid something called DIC, or Diffuse Intravascular Coagulation. Your body has a supply of self-arranging molecules called clotting factors that will attempt to close off breaches of your circulatory system by building a protein scaffold across the gap. This supply is sufficient for most injuries, but profuse bleeding after multiple GSWs can “burn up” your clotting factors and without effective clotting you can’t stop ANY bleeding. Avoid DIC and stop bleeding ASAP, don’t be gentle and don’t worry about causing them pain if they have an arterial pumper. Apologize later, but get control NOW.
The other advice is to not get target-locked on one wound and miss the other one. The logical error there is “satisfaction of search”. Patients are unreliable, particularly when traumatized, they may tell you that they were shot in the hand but not even realize their hand was in front of their chest or abdomen. Finding presumed entry and exit wounds are good, being sure there isn’t a second pair is better. The wound you see may be minor, be sure there aren’t any others.
Wound contamination is not great, but if you take the time to look for sterile supplies the patient might die on the way to the hospital. We can always give antibiotics afterward (it’s standard surgical preparation, in fact). Stop the bleeding however you need to, an occasionally overlooked tool (or so I have read) is the tampon — it’s sterile out of the package, and it’s designed to be put in a cavity & absorb blood. Clean towels, a dirty T-shirt, whatever you have to get pressure on and around the wound is better than doing nothing.
That was interesting. I was actually unaware of the ‘burn of clotting factors’ issue. The ‘satisfaction of search’ issue is big. The liver? A .22LR in the liver is often fatal, which is remarkable. One year ahead of me in law school, a student was shot gratuitously by 12-year-old muggers (on Capitol Hill) after he gave up his wallet. They hit his liver. He died an hour or so later. I’d think a DVD would be an excellent way to deliver refreshable detailed gunshot trauma first aid instruction. Have you come across any?
To be honest, I haven’t looked.
Great post, Darren. I had to do an emergency tracheotomy on an accident victim years ago. Motorcylist; hit from behind, open face helmet. Landed face down on the widshield of the car that him, split his jaw bone and stuck half of it in his throat.
I have been carrying tampons and sanitary napkins in my first aid ruck for years – they’re designed to absorb and contain fluids. Those, and duct tape. I also carry Kwik Clot, trauma pack and individual dressings.
Had a vascular surgeon give me great compliments on wound management after a motorcycle wreck once, and offered to train me to a greater degree. Good advice.
Does this book cover blade injuries? Blunt trauma?
Dunno if it does or not, but stab wounds and GSWs are in the penetrating injury category (and statistically, people survive handgun GSW and stab wounds with identical frequency).
Blunt trauma is, at least in medicine, a separate proposition.
Blunt trauma often involves internal bleeding and without being trained specificly to deal with those types of injury you are often SOL till the trained profesionals arrive.
First aid is important, especially with GSW’s, but I think we need to remember that the chances of a GSW are low compared to other mundane injuries and medical conditions. Don’t forget to learn the rest of first aid!
Thank you, everyone, for your kind comments, and to Eric for posting this review. This is definitely a unique “first aid” book, and the class that goes along with this book will give you tremendous hands-on experience with the skills discussed. As mentioned above, the skills learned from the book and class certainly are applicable to trauma of other sorts, and not just GSW’s. We hope this book saves lives.
Great topic! You are more likely to save a life with your medical skills than take a life with your shooting skills.
Lots of people are curious about what to put in a blow out kit. Folks, if you’ve got to ask, then stick with the basics… band-aids and an Israeli Battle Dressing (The “Emergency Bandage” from Persys Medical (sp?)).
The Israeli Battle Dressing is a very effective bandage that can even be self-administered. Watching a YouTube ‘how to’ video and practicing with one on a friend will give you enough of the fundamentals of treating a GSW until medics arrive if you haven’t received any other training.
Once you’ve received additional hands-on training, you’ll be better equipped to know whether you need other medical devices (such as the naso tubes) in your kit.
My full kit has a whopping five things in it: a CAT tourniquet, an IBD, three strips of tape, a tension pneumothorax needle (whatever the hell it’s called) and a naso tube. Frankly, I think I’m way over-prepared but it all sits quietly in my map pocket in the door of my car ready for use at a range or in real life.
During classes, I carry an IBD.
As with firearm training: A bad first-aid class beats the best book or video for training. Seek out first aid training just as you would seek out training in how to *fight* with your handgun (and long-gun). Doesn’t matter if it’s a class taught by the folks who put together this book or one of Doc Gunn’s classes or another similar instructor, get some first aid training.
The life you save might be your own.
I couldn’t agree more with your encouragement for people to go take a class. This book is best supplemented with actual hands-on training by people who can teach you how and why certain things should be done (or NOT done) in order to save a life when seconds count. Thanks!
I have purchased a copy of the book and have since taken Red Cross EMR training and I’ve found that while the Red Cross EMR (Emergency Medical Responder- essentially EMT-lite) training is very clinical, the book takes most of the same things I learned and puts them into a real-world scenario.
EMR training assumes a safe scene, but being in a gunfight is anything but. Dr. Meade’s book stresses finishing one job (the fight) before doing any patch-up work, which sounds obvious, but isn’t. Head, neck, and spinal injuries are paramount to an EMR, but a firefight is about living thru it which means you might have to drag someone with a potential HNS injury to safety. If I had not had the EMR training, the info on wound stuffing and wrapping, tourniquets, and PTX would have been the first introduction I’d had to it and definitely worth the price of a book.
Is it perfect? No, nothing is. I stopped marking spelling and punctuation errors in it about half way thru. However the info is drawn from real world experience (which I have little of in this arena) and presents it in a very down-to-earth manner and sets it up in a fashion that anyone can understand and use.
While I have no qualifications in the medical arena beyond my EMR certification, none of the info in the book appears to be incorrect, misleading or liable to do more damage than what it tries to help you fix. For a layperson, it distills everything down to useful info any CCW operator should have in his library and bag of tricks. Heck, the “move to cover” bit even helped me with the final practical EMR test. I would recommend this book to anyone who carries or has an interest in it.
Look folks, this book is NOT the end all be all as it is a short manual. Don’t rely on a book as a replacement for hands on training. Get out there and train and put the book down!
At a price of $25.00 this book is NOT worth your hard earned money. Suarez is legally stealing your money. To boot, his little gang of followers will blindly stand up for Gabe and his thief-like tactics.
The information in the book is okay but not worth $25.00. Also, you can research everything that is in this book online for FREE.
Ok, I understand you don’t think this is a good buy, but why the hostility? And what does Gabe Suarez have to do with this?
As a female trauma surgeon and gun enthusiast I do not recommend this book. It is a short manual that lacks so much information. A little knowledge can be more dangerous than beneficial. Skip this one.
Dr. Prokiski,
Have you read the book? Please share with me what information you feel a non-medical person would require to provide immediate first aid for GSW’s and other penetrating trauma, that we did not provide in this short book? This is not a book designed for the ambulance, the Emergency/Trauma Center, or the operating room. I am truly interested in what you feel is missing, especially given the fact that the person who wrote the review is also a surgeon, and liked the book.
“As a female trauma surgeon”
Can you please elaborate on your qualifications Doctor? The AMA has no record of any doctor in the US or PR with that spelling, and the only doctor I can find with similar spelling is an Orthopedic Surgeon, is that you? I only ask since you specifically started your post by stating that you are a trauma surgeon and then offered advise, as such I am interested in your qualifications.
You would probably have better luck searching in state medical boards databases. The AMA is a private organization that not all doctors are a member of, and the “doctor finder” services are not exactly reliable. Not being a member of an organization doesn’t mean anything really.
Where’s Nick Leghorn at? As someone who used to be an EMT in a major urban area I am interested to see what Nick’s (an EMT) take on the book is.
To the authors I would like to say thank you for writing a book like this. Many of us go into remote locations to shoot and in the case of an accident our likelihood of survival can rest solely on the person with us. There is always the chance that if I am injured I will not be coherent enough to talk who ever is with me through what needs to be done. Once I get a chance to read it myself this will most likely go on my must read list for all sportsman and range regulars.
Also, since “sucking chest wounds” have been mentioned a couple of times, I feel I would be remiss if I did not bring up the old medic pun that all chest wounds suck.
A podcast interview with me to discuss my book and classes was just released. Those who want to hear more about it might enjoy listening.
http://www.handgunworld.com/?p=878
For those interested, the authors are now available at http://paragonpride.com/forum
and are always willing to field questions and comments about the book.